
Case date: 6 August 2025
Abstract
We present a case of intravascular lithotripsy (IVL) for a 75-year-old female patient with a history of an abnormal cardiac condition and chronic kidney disease. The patient presented with a near CTO across two lesion sites on the LAD. A 3.50mm IVL catheter was used, delivering a total of 80 pulses to the two lesion sites. The procedure was performed by Dr. dr. Doni Firman, Sp.JP(K), FIHA and dr. Arwin Saleh Mangkuanom, Sp.JP (K), FIHA at RSJPD Harapan Kita. Additional treatments with a conventional NC balloon and stent implementation were utilized. The treatment resulted in significant reductions in stenosis levels. This case highlights the role of IVL in managing complex calcified vascular lesions.
Case Presentation
A 75-year-old female with a medical history of abnormal cardiac condition, requiring the use of a pacemaker and chronic kidney disease, which required the patient to undergo a hemodialysis procedure prior to the IVL treatment, presented with heavy stenosis at the LAD.
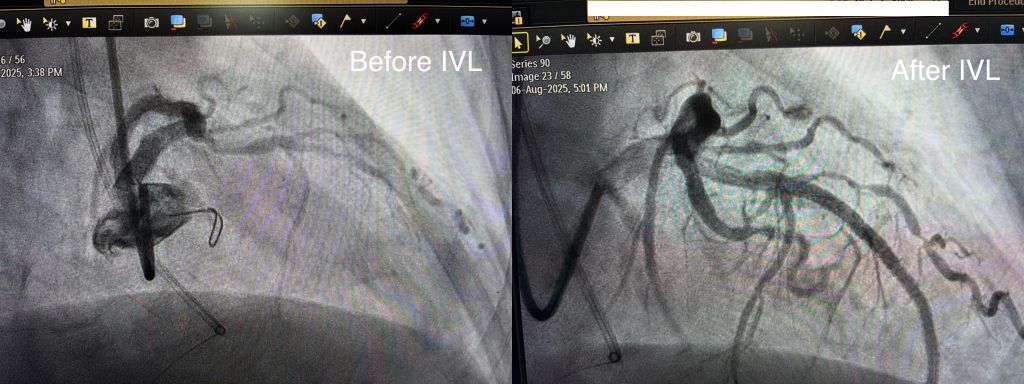
IVUS and angiographic imaging revealed near CTO across two lengthy lesions on the LAD.
The intervention was performed by Dr. dr. Doni Firman, Sp.JP(K), FIHA and dr. Arwin Saleh Mangkuanom, Sp.JP (K), FIHA. at RSJPD Harapan Kita. After a lengthy and challenging procedure to install a guidewire for the IVL balloon to pass through. A 3.50mm Sonico-CX IVL catheter was subsequently advanced across the two lesions. A total of 80 pulses were delivered.
Following the IVL treatment, IVUS and angiographic imaging showed minimal residual stenosis. The vessel was further dilated using an NC balloon, followed by a stent implementation to ensure long-term vascular health.
Outcome
The whole procedure was free of any incidents and highly successful, resulting in the significantly improved vascular health. At follow-up, the patient remained free of any post-surgical complications.
Discussion
This case demonstrates the effectiveness of IVL in treating heavily calcified coronary lesions. Compared to conventional lesion modification strategies such as rotational atherectomy or cutting balloons, IVL provides low risk of dissection and ease of use.
In this patient, the narrow crossing profile of the Sonico-CX catheter allowed for its successful deployment on the heavily calcified lesion sites and forgo the need to use rotational atherectomy, which was considered at one point during the procedure. Our experience supports the role of IVL as a valuable tool in managing complex calcified disease, particularly in patients with other pre-existing conditions that require the use of a pacemaker and constant hemodialysis procedures.
Conclusion
Intravascular lithotripsy is a safe and effective method for modifying vascular calcium and optimizing outcomes in patients with complex calcified lesions. This case highlights its potential role as a frontline therapy in selected patients.
Leave a Reply